Laparoscopic Highly Selective Vagotomy (partial cutting of vagus nerve)
A. The Condition. You may have an ulcerous condition of the stomach or duodenum in which surgical treatment is recommended. The vagus nerve controls acid secretion in your stomach. Cutting some of the vagal nerves (“highly selective”) to the stomach reduces acid production, which allows your ulcers to heal.
B. Symptoms
- Abdominal pain, especially at night
- Weight loss, weakness
- Vomiting blood
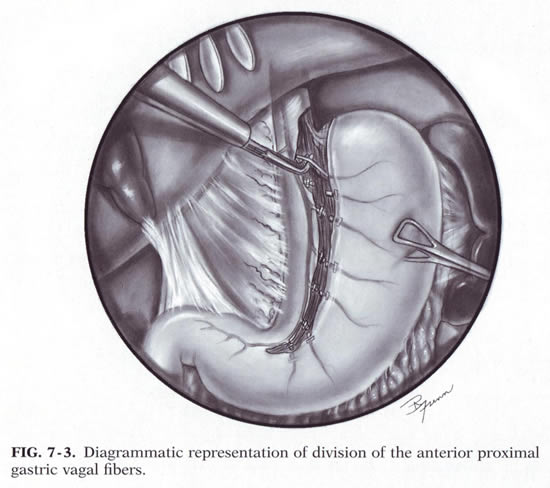
C. Laparoscopic Highly Selective Vagotomy. The surgeon will make about 4-5 small incisions in your abdomen. A port (nozzle) is inserted into one of the slits, and carbon dioxide gas inflates the abdomen. This process allows the surgeon to see inside of your abdomen more easily. A laparoscope is inserted through another port. The laparoscope looks like a telescope with a light and camera on the end so the surgeon can see inside the abdomen. Surgical instruments are placed in the other small openings and used to cut some of the vagal nerves to the stomach. These nerves go to the proximal portion of the stomach. After this has been accomplished, the carbon dioxide is released out of the abdomen through the slits, and then these sites are closed with sutures or staples, or covered with glue-like bandage and steri-strips.
Dr. Frantzides was the first in the world to report a Laparoscopic Highly Selective Vagotomy in 1992.
D. Nonsurgical Treatment. Sometimes your problem may be treated with medication (antacids and/or various medicines that reduce acid production in the stomach). Your doctor will discuss with you what your best option is.
E. Risks. The primary risks of laparoscopic highly selective vagotomy are:
- Infection of the skin at one of the small ports sites
- Perforation of the stomach
- Slow emptying of food from the stomach
- Postoperative ileus (the intestines slow down/stop working for several days)
F. Expectations
1. Before Your Operation. Laparoscopic highly selective vagotomy usually is an elective procedure. The preoperative evaluation might include blood work, urinalysis, a barium swallow x-ray, and endoscopy (looking down your throat with a scope). If you smoke, then you should stop immediately. If you are taking blood thinners (for example, aspirin, coumadin, Lovenox, or Plavix), then you will need to stop these one week prior to your procedure. Your surgeon and anesthesia provider will review your health history, medications (including blood thinners), and options for pain control.
2. Your Recovery. You usually can go home 1-2 days after a laparoscopic highly selective vagotomy. You may need to wait until your bowels start working. You will be given medication for pain. Your doctor will discuss with what to do with your anti-ulcer medications. You should limit your activity to light lifting (no more than 15 lb) for one month.
3. Call Your Surgeon if you have one or more of the following:
- High fever
- Severe abdominal pain
- Odor or increased drainage from your incision
- Nausea and vomiting
- No bowel movements for three days
G. Pertinent References
Frantzides CT, Ludwig KA, Quebbeman EJ, Burhop J. Laparoscopic highly selective vagotomy: technique and case report. Surg Laparosc Endosc. 1992 Dec;2(4):348-52.
Frantzides, C.T.: Laparoscopic Vagotomy. In Laparoscopic and Thoracoscopic Surgery. Ed. Frantzides, Mosby Year-book Inc. 1994
Frantzides CT, Carlson MA. Laparoscopic highly selective vagotomy. J Laparoendosc Adv Surg Tech A. 1997;7(3):143-6.