Laparoscopic Colectomy (Large Bowel Resection)
Colon Diseases:
Numerous colon and rectal problems are amenable to laparoscopic resection. Problems related to Inflammatory Bowel Disease (such as Crohn’s or Ulcerative Colitis), Familial Polyposis, volvulus (twisting of the bowel), endometriosis, diverticular disease and other benign and malignant diseases of the colon can be treated with minimally invasive surgery.
Dr. Frantzides is a pioneer in laparoscopic colorectal surgery and has been performing minimally invasive procedures upon the colon both for benign and malignant diseases. He was the first in the world to perform a laparoscopic correction of malrotation of the colon in 1996.
Symptoms:
The symptoms associated with benign and cancerous colon disease vary widely but include the following:
- Blood in stool
- Abdominal distention
- Abdominal pain
- Thinned (pencil-like) stools
- Obstruction
Diagnosis:
Several studies can help your doctor make decisions:
- Endoscopy (video surveillance)
- Rule out cancer
- Evaluate for inflammation
- Diverticular disease
- Polyps
- Tissue biopsy
- Barium enema
- Rule out cancer
- Kinking or twisting of the colon
- Stenosis or blockage
Surgery:
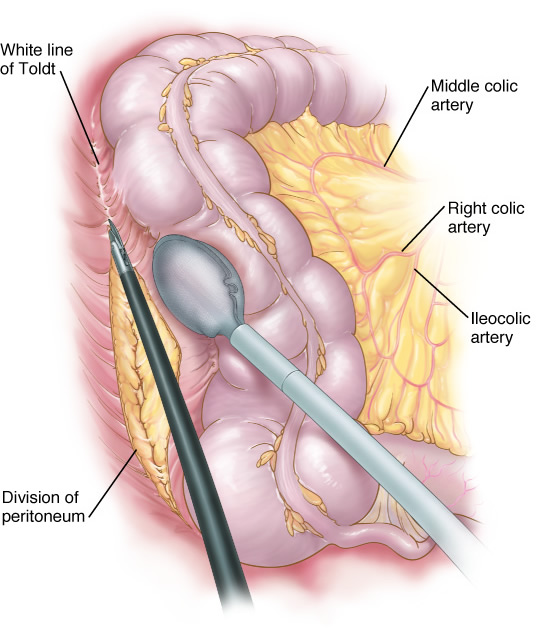
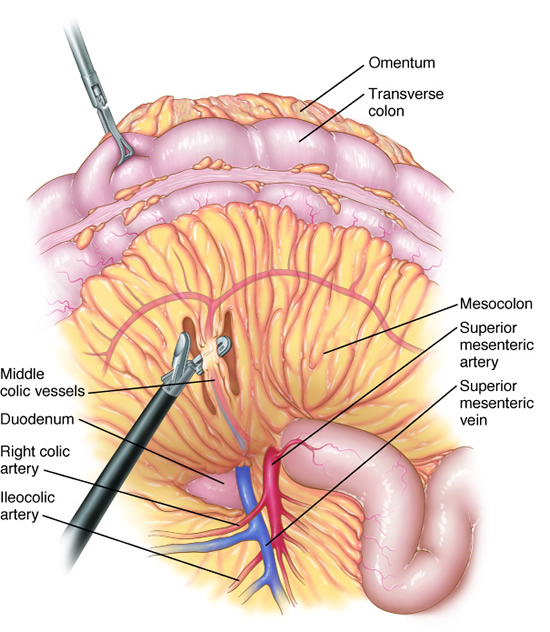
Laparoscopic colectomy is feasible for benign and cancerous lesions. Rectal cancers that are more than 5 cm above the end of the rectum may also be resected (low anterior resection) with preservation of continence. Dr. Frantzides has been performing laparoscopic colectomies since 1992 and he has operated on patients with complex colorectal ailments. (See Patient Stories)
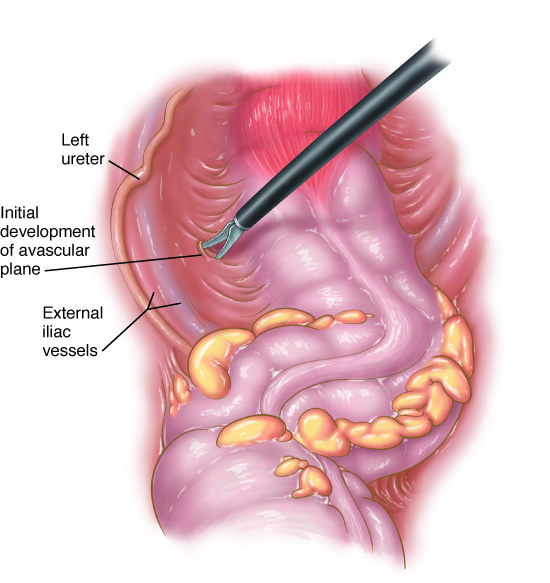
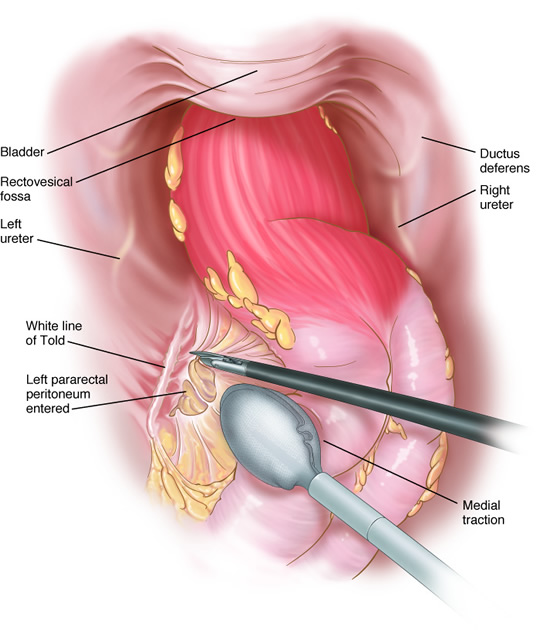
Open surgical approach requires an 8-inch incision on the abdomen. The laparoscopic approach involves making four half-inch incisions on the abdomen through which a camera and three instruments are placed. The colon to be resected is mobilized. One of the port sites is enlarged slightly and the colon is removed.
Procedures:
The principals involved in removing portions of the colon are similar for many different operations involving benign and malignant disease. Procedures that may be performed laparoscopically include:
- Segmental colectomy
- Ascending colectomy (and ileocolectomy)
- Sigmoid colectomy
- Total abdominal colectomy
- Total proctocolectomy (whole colon and anus)
- Abdominoperineal resection (rectum and anus)
- Rectopexy (rectal prolapse)
Recovery:
Patients recover much sooner after laparoscopic surgery. Return to activities can occur within three to seven days compared to 2-4 weeks with an open approach. Wound infections and hernias occur less frequently with the laparoscopic technique. Also, much less pain has been reported with laparoscopic surgery.
Pertinent References
Frantzides, C.T., Luu, M., Welle S., Laparoscopic Ileocecectomy for Complicated Inflammatory Bowel Disease. Video Atlas of Advanced Minimally Invasive Surgery. Sounders Elsevier 2013
Frantzides, C.T., Welle S., Laparoscopic colectomy for divericulitis and colovesical fistula. Video Atlas of Advanced Minimally Invasive Surgery, Sounders Elsevier pp 211-216; 2013
Frantzides, C.T., Madan AK, Carlson M, Zografakis JG, Zeni TM Mieselman M, Roberts J, Ayiomamitis G.; Laparoscopic Colectomy in an Academic U.S. Center; Hellenic journal of Surgery 81 (4):80-86,2009
Frantzides, CT, Carlson M, Polymeneas G; Laparoscopic Sigmoid Colectomy; In Atlas of Minimally Invasive Surgery. Frantzides, Carlson (ed.) Elsevier 2008.
Frantzides, CT, Carlson M, Laguna L; Laparoscopic Transverse Colectomy; In Atlas of Minimally Invasive Surgery. Frantzides, Carlson (ed.) Elsevier 2008.
Carlson MA, Frantzides CT: Canine myoelectric activity after open versus laparoscopically assisted right hemicolectomy. Am J Surg, 174: 79-82, 1997.
Wittmann DH., Schein M., Frantzides CT: Diverticulitis. In SL Gorbach, JG Bartlett, NR Blacklow (Eds) Infectious Diseases in Medicine and Surgery. W.B. Saunders. Second Edition pp. 828-833, 1997
Carlson MA, and Frantzides CT. Resolution of Ileus after open versus laparoscopically-assisted right hemicolectomy in the dog. Proceeding of the XXXVIII SSAT, 1996.
Frantzides CT, Carlson MA: Minimally invasive surgery of the colon and rectum. Proceedings of the 15th World Congress of Collegium Internationale Chirurgiae Digestivae, J.P. Kim and R.E. Condon Ed. Monduzzi Editore, Bologna, Italy, pp 39-45, 1996.
Frantzides, CT, Cziperle, DJ, Soergel, K, and Stewart, E: Laparoscopic Ladd Procedure and Cecopexy in The Treatment of Malrotation Beyond the neonatal period. Surg Laparosc Endosc. 6:73-75, 1996.
Wittmann, D.H. and Frantzides, C.T.: Diverticulitis. In Infectious Diseases. Gorbach, S., Bartlett, J. and Blacklow, N., Eds. Saunders Co., pp. 682-687, 1992.
Carlson, M.A., Ludwig, K.A., Cowles, V.E., Frantzides, C.T., and Condon, R.E.: The effect of propranol on human colonic myoelectric activity in the postoperative period. Gastroenterology 103:1382; 1992.
Ludwig, K.A., Carlson, M.A., and Frantzides, C.T.: Does minimally invasive surgery result in a shorter period of postoperative ileus? Gastroenterology 103:1382; 1992.
Ludwig, K.A., Frantzides, C.T., Cowles, V.E., Carlson, M.A., and Condon, R.E.: Cholecystokinin and gastrin responses during postoperative ileus. Gastroenterology 103:1382; 1992.
Condon, R.E. and Frantzides, C.T.: Physiology of the colon, rectum and anus. In Operative Colorectal Surgery. Block, G.E. and Moosa, A.R., Eds. W.B. Saunders Company, 1994.
Carlson, M.A., Frantzides, C.T.: Resolution of postoperative ileus in laparoscopic vs open colectomy. J Gastroenterol Hepatol 10:84, 1995.
Frantzides, CT, Cziperle, DJ, Soergel, K, and Stewart, E: Laparoscopic Ladd Procedure and Cecopexy in The Treatment of Malrotation Beyond the neonatal period. Surg Laparosc Endosc. 6:73-75, 1996.